2003年 Lee et al [5]對於其疼痛產生原因解釋為-疼痛機制為髕骨向外側位移(lateral glide)和傾斜(lateral tilt),使得髕骨與股骨接觸面積減少(contact area decrease),因此當人體做負重活動時接觸面積減少,PatellofemoralJoint仍需承受同樣的力(force),使關節間壓力增加而產生疼痛。同年2003年Powers et al [8]與2008年Bolgla LA [6] 提出當下肢執行承重活動(weight-bearing activities)時,髕骨股骨疼痛症候群(PFPS)的個案經常產生過多的股骨內轉(femoral internal rotation),導致髕骨相對的向外側位移與傾斜。然而髕骨股骨疼痛症候群(PFPS)患者主訴經常是在下肢承重的情形下才有疼痛情況,因此2003年Robinson et al [10]研究其結果-影響承重情況下膝關節控制性的重要因素是髖關節週邊肌群,並明確的提出女性髕骨股骨疼痛症候群患者的髖外展肌群(hip abductors)與髖外轉肌群(hip lateral rotators)皆有顯著肌肉無力型態。近年來諸多研究者已經認知到不正常的髖關節活動將導致股骨在額面(frontal plane)與水平面(transverse plane)上有過多的動作,且由於人體動力鏈(Body kinetics)關係,易造成動態膝關節過多的外翻(dynamicexcessive valgus)。不正常髖關節活動導因為何,在2008年Bolgla LA [6]與2009年Prins和Wurff [9]針對髕骨股骨疼痛症候群患者髖關節肌力測試並做出結論,髖關節外展肌( hip abductors)、外旋肌( hip external rotators)、和伸直肌(hip extensors)有明顯的肌力缺損,但許多學者研究仍以髖關節外展肌( hipabductors)和外旋肌( hip external rotators)在動態活動與靜態活動上有顯著的肌力缺失認定為主要原因。
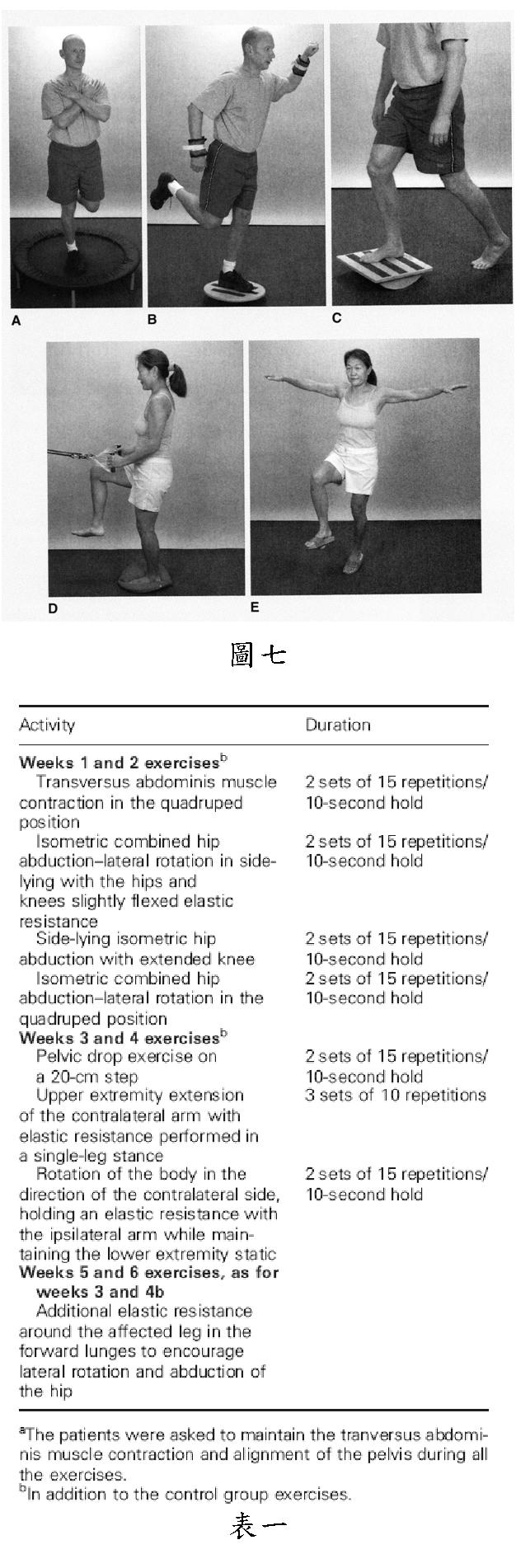
確認明顯肌力缺損後,2008年Nakagawa et al [7]在實驗組進行腹橫肌(transverse abdominals)、髖外展肌群(hip abductors)及髖外旋肌群(hip lateral rotators)肌力訓練與功能性訓練,經由1星期訓練5次,其中1次由治療師監督運動方式可否正確另4次在家自行訓練,訓練持續6週;在疼痛改善、膝伸直力矩(knee extension torque)、臀中肌的EMG活動上都有改善,作者提及雖然腹橫肌(transverse abdominals)的肌力訓練能改善功能性活動,但支持的論點仍尚未明確,作者建議未來能再更進一步追蹤。2010年Fukuda et al [11]更針對運動治療方式做出比較,實驗組髕骨股骨疼痛症候群患者同時肌力訓練髖關節與膝關節肌群,控制組僅以傳統訓練髕骨股骨疼痛症候群患者膝關節肌群及對髕骨做關節鬆動術為主,經過每星期3次且為期連續4星期運動治療;在實驗組與控制組相較之下,實驗組患者疼痛與日常生活功能性活動都有顯著改善。
因此要重建正常下肢動力學( kinematics of lower extremities)才可將髕骨股骨疼痛症候群(PFPS)治癒並期待不再次發生。
三、運動治療計畫( 2008 Nakagawa et al[7], 2010 Kirsty Mckenzie et al [4], 2010 Eduardo Magalhães et al[2] )
3.Hertling Kessler.Management of Common Musculoskeletal Disorders: Physical Therapy PrinciplesMethods. 2006 4thEdition
4.Kirsty Mckenzie, Victoria Galea, Jean Wessel, Michael Pierrynowski. Lower extremity kinematics offemales with patellofemoral pain syndrome while stair stepping. J Orthop SportsPhys Ther 2010;40(10): 625-632
5.Lee TQ, Morris G,Csintalan RP. The influence of tibial and femoral rotation on patellofemoralcontact area and pressure. J Ortho Sports Phys Ther. 2003;33:686-693
7.Nakagawa TH, Muniz TB, Baldon Rde M, Dias Maciel C, de Menezes Reiff RB,Serro FV. The effect of additionalstrengthening of hip abductor and lateral rotator muscles in patellofemoralpain syndrome: a randomized controlled pilot study. Clin Rehabil.2008;22:1051-1060
8.Power CM. Theinfluence of abnormal hip mechanics on knee injury: a biomechanicalperspective. J Orthop Sports PhysTher 2010;40(2):42-51.
9.Prins MR, Wurffvan der P (2009) Females with patellofemoral pain syndrome have weak hipmuscles: a system review. Australian Journal of Physical therapy 55: 9-15
10.Robinson RL, NeeRJ. Analysis of hip strength in females seeking physical therapy treatment forunilateral patellofemoral pain syndrome. J Orthop Sports Phys Ther. 2007;37:232-238